The AEROCHAMBER PLUS® FLOW-VU® AVHC
Using your inhaler with the AEROCHAMBER PLUS® FLOW-VU® chamber decreases the amount of aerosol from the inhaler that lands in your mouth, which can cause drug side effects. Use together to help get more medication deeper into your lungs where it needs to be to work the best.
AEROCHAMBER PLUS® brand of chambers delivers the intended dose established by the pharmaceutical company. Use of other chambers may lead to medication waste, less than optimal doses, and varying therapeutic responses.
For respiratory patients, getting the most from life means getting the most from their inhaler medication.
Each chamber has special features to work best for the user.
- Small and medium mask chambers include a sensitive valve for kids and babies who don’t take in big breaths.
- Three chambers (mouthpiece, intermediate, and large masks) have a FLOWSIGNAL® Whistle. If the breath in is too fast, the whistle will sound to let you know to slow down.
- Each of our masks are specifically designed to fit the shape of the face with no leaks around the edges.





How It Works
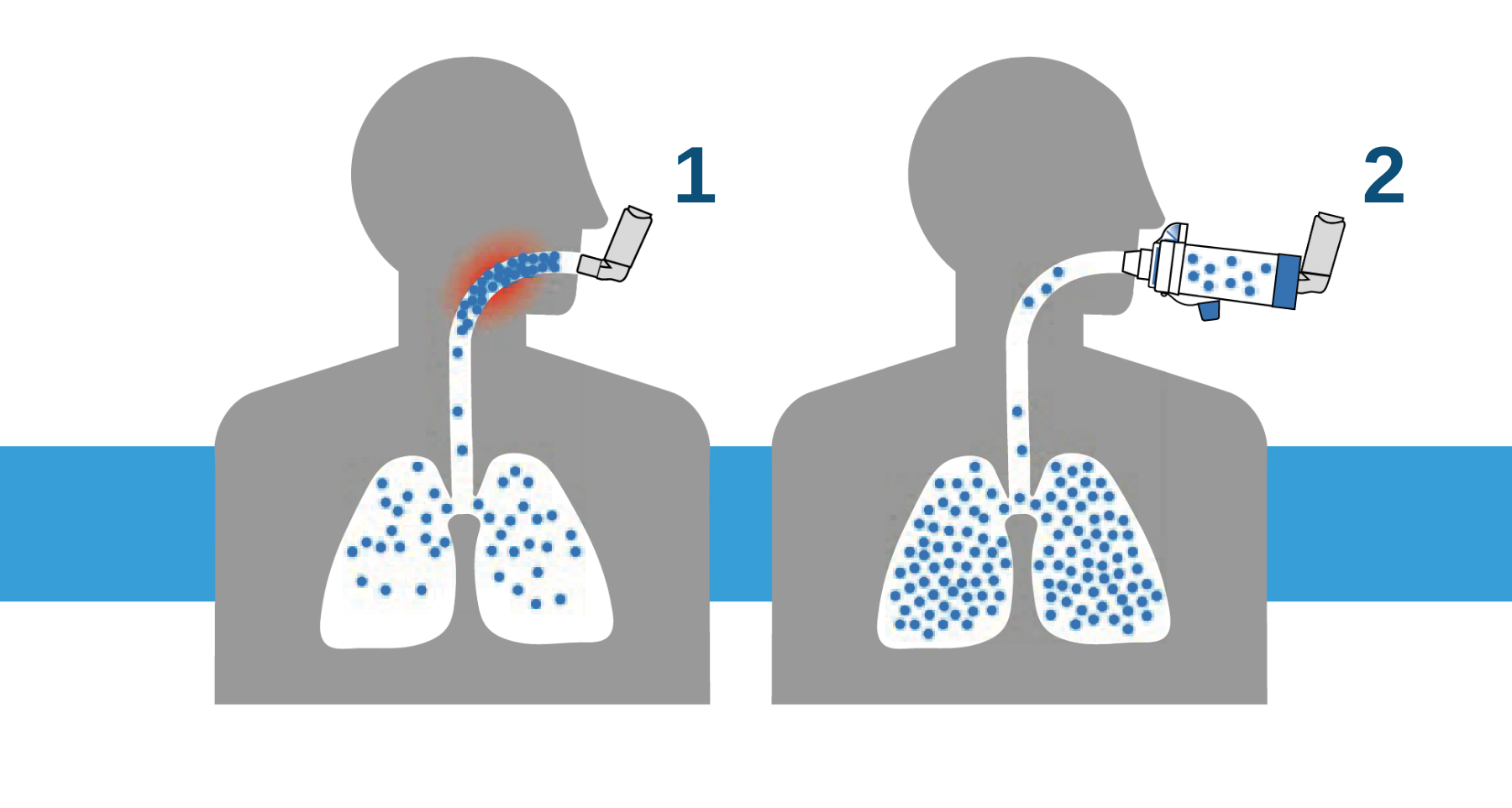
- Inhaler alone with poor technique. Poor lung delivery means you can taste your inhaler medication.
- Inhaler with AEROCHAMBER® brand of chamber. People who use our chamber with their inhaler have better control.1
1Nagel M, et al. CSACI 2017
How To Use
Using your inhaler with the AEROCHAMBER PLUS® FLOW-VU® chamber decreases the amount of aerosol from the inhaler that lands in your mouth, which can cause drug side effects. Use together helps get more medication deeper into your lungs where it needs to be to work the best.
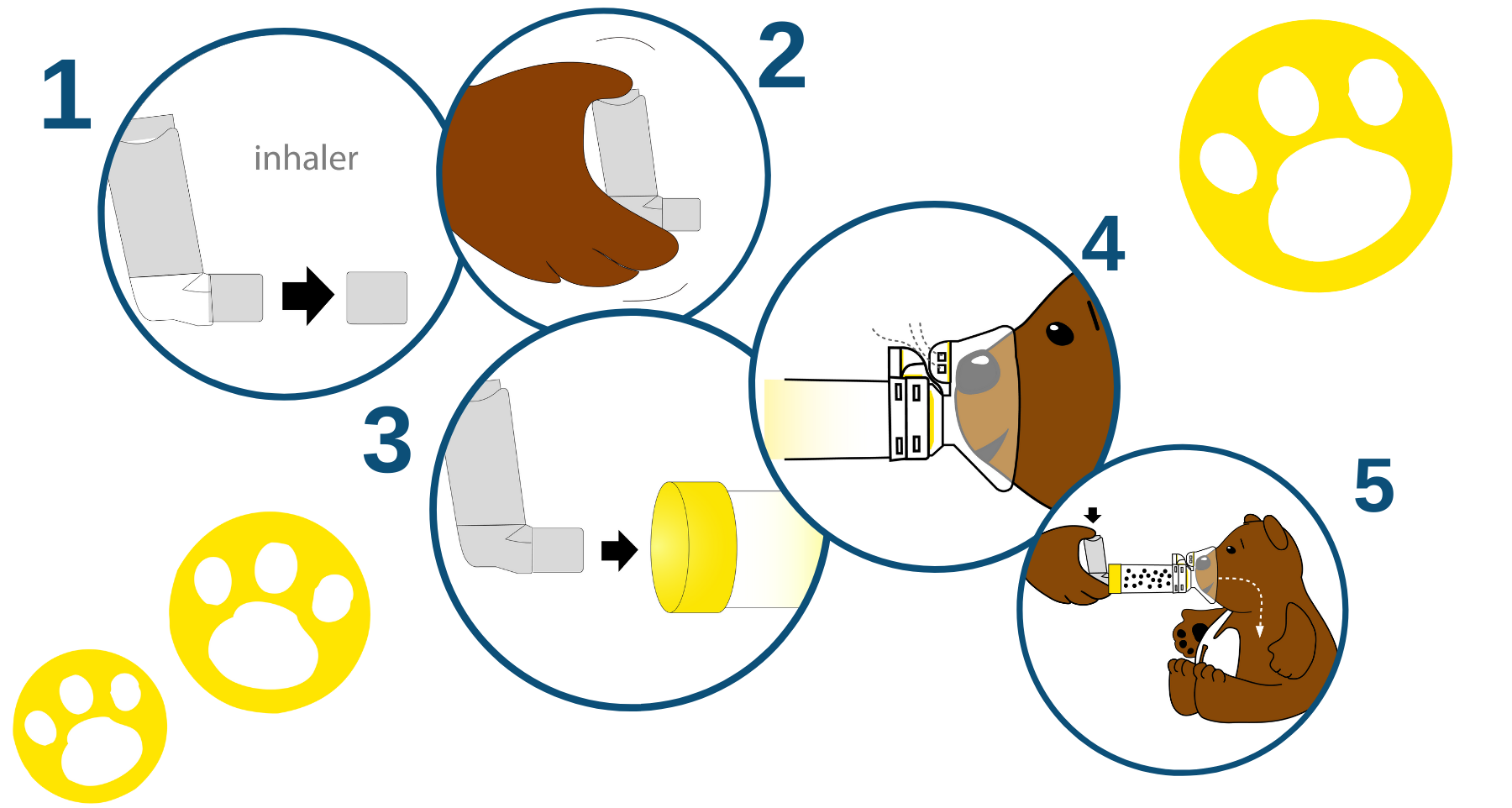
- Remove the inhaler cap.
- Shake the inhaler.
- Insert the inhaler into the back of the chamber.
- Apply mask to face.
- Press inhaler and count for 5 to 6 breaths.
These are shortened user instructions. Always review the complete instructions packaged with the chamber.
Frequently Asked Questions

HOW DO I DETERMINE WHICH MASK SIZE TO USE?
The top of the mask should sit on the bridge of the nose and the bottom should rest between the bottom of the lips and the chin. Contact your Territory Manager for details.
DO YOU OFFER INTERCHANGEABLE MASKS FOR YOUR CHAMBERS?
No, the chamber and mask combinations are specifically designed to optimize medication delivery for the individual need of each patient. The small and medium chambers have inspiratory valves that are specifically designed for lower flow rates, so they open easily for infant or pediatric patients especially when tidal breathing. The intermediate and the large chambers are also equipped with the FLOWSIGNAL® Whistle to alert the user when they are inhaling too quickly and to encourage slower deeper breaths.
WHY WOULD I NEED TO USE A CHAMBER WITH A SOFT MIST INHALER FORMAT?
Although the aerosol plume generated by a soft mist inhaler is slower than an MDI, one of the biggest challenges with using an inhaler alone is proper inhalation technique. In order to get the most from an inhaler, whether a traditional metered dose or soft mist inhaler, the patient must begin inhaling before they press the inhaler and continue to inhale long enough to get the medication to their lungs. AEROCHAMBER PLUS® FLOW-VU® aVHC is the FIRST valved holding chamber FDA Cleared for use with Soft Mist Inhalers.
HOW OFTEN SHOULD THE CHAMBER BE CLEANED?
The AEROCHAMBER PLUS® FLOW-VU® Chamber should be cleaned once a week. The chamber is easy to take apart to clean in either the dishwasher or using soap and water.
HOW OFTEN SHOULD THE CHAMBER BE REPLACED?
The AEROCHAMBER PLUS® FLOW-VU® Chamber should be replaced every 12 months. However, you should replace it if any of the following occur (1) The valves are missing or damaged. When this happens, the chamber cannot work properly and must be replaced. (2) The back piece becomes cracked or torn. This may affect the amount of drug that is breathed in. (3) The mask does not comfortably fit the face. It may be time to use another model with a larger mask or use the AEROCHAMBER PLUS® FLOW-VU® aVHC with mouthpiece.
WHAT IS THE FLOW-VU® INHALATION INDICATOR?

The AEROCHAMBER PLUS® FLOW-VU® Chamber is the only chamber with a dedicated inhalation indicator. The FLOW-VU® Inhalation Indicator is a valuable feedback tool on the AEROCHAMBER PLU® FLOW-VU® Chamber that moves as the user breathes to confirm correct use and medication delivery. The FLOW-VU® Indicator is especially useful for parents who are giving the inhaler medicine to their children. The indicator lets you count the number of breaths your child takes through the chamber and helps you to know the medication was given correctly.
CAN THE CHAMBERS BE USED WITH INHALERS LIKE QVAR† WITH THE ROUND END?
Yes. The AEROCHAMBER PLUS® FLOW-VU® Chambers can be used with ALL commonly prescribed metered dose inhalers. They are the most recommended chamber by leading metered dose inhaler pharmaceutical companies.
CAN THE CHAMBERS BE USED WITH SOFT MIST INHALERS LIKE SPRIRIVA†?
Yes. The AEROCHAMBER PLUS® FLOW-VU® Chambers are FDA cleared for use with both metered dose inhalers and soft mist inhalers. Download the product insert for step-by-step instructions.
WHAT DOES ANTI-STATIC MEAN AND WHY IS IT IMPORTANT?
Many things can have a type of static electricity that makes other things stick to it, for example rubbing a balloon over hair can create static. Anti-static materials decrease the static charge or “clinginess” to a surface. This is very important to have so that the medication does not stick to the walls of the device but can go into your lungs where it needs to be.
IS THE AEROCHAMBER PLUS® FLOW-VU® CHAMBER ANTI-STATIC?
Yes, all of the parts (including the masks) are made with an anti-static polymer that is built into the chamber and is special to the AEROCHAMBER® devices. Static will never build up on these devices (even if stored in a plastic bag) and they can be used straight from the package without washing.
DOES THE AEROCHAMBER PLUS® FLOW-VU® CHAMBER CONTAIN BPA?
None of our chambers are made or manufactured using BPA, natural rubber latex, phthalates, lead, or PVC. Our chambers are manufactured in the US using parts from the US and Canada.
WHY WOULD AN ADULT USE A CHAMBER?
The majority of adults do not use their inhalers properly. Up to 80% of people have poor inhaler technique which can lead to asthma attacks and poor outcomes.1
Chambers help by making it easier to inhale your medication and helping to ensure the inhaler medication is delivered to your lungs, where it is needed.
1Global Initiative for Asthma 2021
Clinical Evidence
AEROCHAMBER PLUS® FLOW-VU® AVHC CLINICAL EVIDENCE SUMMARY
Only AEROCHAMBER PLUS® FLOW-VU® chambers were equivalent to the reference device data listed in virtually all innovator inhalers currently approved in the US and European markets. Differences in chamber design, materials and function mean that chambers should not be automatically considered interchangeable. Learn more.
VALVED HOLDING CHAMBERS ARE NOT ALL EQUIVALENT IN PERFORMANCE AND AS A RESULT SHOULD NOT BE REGARDED AS INTERCHANGEABLE
Only AEROCHAMBER PLUS® FLOW-VU® chambers were equivalent to the reference device data listed in virtually all innovator inhalers currently approved in the US and European markets. Differences in chamber design, materials and function mean that chambers should not be automatically considered interchangeable. Learn more.
DIFFERENT CHAMBERS DELIVER DIFFERENT AMOUNTS OF MEDICATION WHICH CAN LEAD TO MEANINGFUL DIFFERENCES IN CLINICAL PERFORMANCE
The author found that it was unequivocal that differences exist between different chambers which in a number of cases are sufficiently large that meaningful and overt clinical differences would be anticipated as a result. Learn more.
A COMPARATIVE ANALYSIS OF CHANGES IN PMDI DRUG DOSE DELIVERY BEFORE AND AFTER DETERGENT COATING USING FIVE ANTISTATIC VALVED HOLDING CHAMBERS
Some “antistatic” valved holding chambers (aVHC) have poor antistatic properties and should therefore be considered non-antistatic and primed. Differences in antistatic properties are an important cause of the large performance differences between aVHCs. Learn more.
References:
1Levy et al. Prim Care Respir J. 2013;22(4):406-11.
2Nagel M, et al. CSACI 2017